The Bristol Stool Scale: Clinical Physiology and Transit Time Analysis
An in-depth guide to the global medical standard for assessing colonic function and digestive morphology.
Origins and Clinical Purpose
If you've ever seen a doctor about digestive issues, you've probably encountered the Bristol Stool Scale — also known in medical literature as the Meyers Scale or the Bristol Stool Form Scale (BSFS). It's a rigorously validated clinical tool used by gastroenterologists, researchers, and dietitians worldwide. It was developed and published in 1997 by Dr. Stephen Lewis and Dr. Ken Heaton at the University Department of Medicine, Bristol Royal Infirmary, with one clear goal: to standardize the highly subjective categorization of human feces.
Before it existed, describing digestive issues was a mess of vague, subjective language — making it genuinely hard for doctors to gauge the severity of what a patient was experiencing. The scale solved that by establishing seven distinct morphological categories, running from severe constipation all the way to acute diarrhea. That gave clinicians a shared, objective visual language. Today it's a cornerstone in diagnosing and managing functional bowel disorders, most notably Irritable Bowel Syndrome (IBS).
The Physiology of Colonic Transit Time
To get why the Bristol Scale matters clinically, it helps to understand what the large intestine (the colon) actually does. Its primary job isn't digestion — that's mostly handled by the stomach and small intestine. The colon's role is to absorb water and electrolytes, and to help synthesize certain vitamins through the gut microbiome. When the liquid slurry of digested food (chyme) arrives from the small intestine, it's heavily saturated with water.
What a stool looks like — its shape and consistency — is almost entirely determined by one thing: how long it spent in the colon. That's colonic transit time. The colon moves waste forward through peristalsis, a series of wave-like muscle contractions, and the entire time, its mucosal lining is pulling water out of the passing material. The longer the transit, the more water gets extracted, and the harder and drier the stool becomes. Flip it around, and a transit that's too fast means the colon doesn't have time to do its job — resulting in liquid, unformed stools.
Detailed Morphological Breakdown
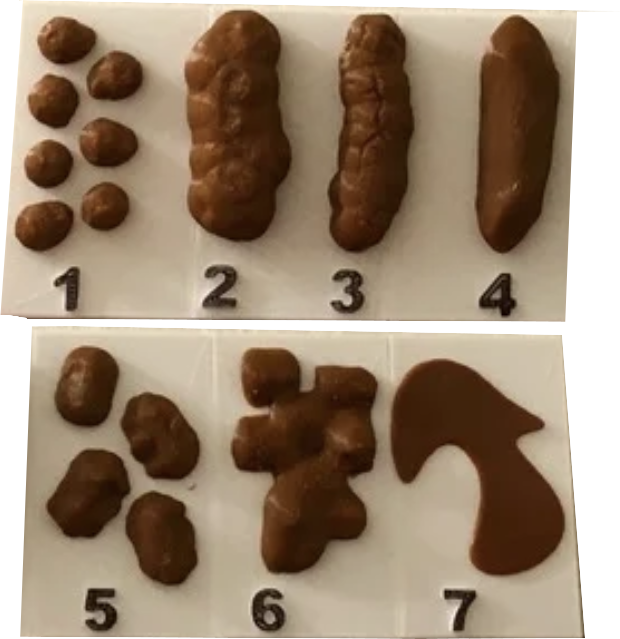
The seven types of the Bristol scale aren't just descriptive labels — they map a spectrum of colonic function, from dangerous prolonged stasis all the way to hypermotility.
Types 1 & 2: Severe and Mild Constipation
Type 1 is characterized by separate, hard, and severely dried-out lumps — often resembling nuts or small pebbles. These indicate a prolonged colonic transit time, sometimes meaning the waste has sat in the bowel for several days. With nearly all moisture extracted, they lack lubrication and frequently require intense straining to pass, which can cause painful micro-tears in the anal canal. Type 2 looks like a single sausage-shaped mass, but its surface is heavily lumpy and compacted. Think of it as a cluster of Type 1 lumps that fibrous tissue has bound together — it's still chronic constipation, just a step less severe.
Types 3 & 4: Optimal Physiological Function
Type 3 keeps the sausage shape but shows distinct cracking on its surface — transit time is a touch slow, but hydration is generally acceptable. Type 4 is the clinical ideal: a smooth, continuous, sausage or snake-like form. That consistency points to a well-calibrated transit time (typically 24 to 72 hours), optimal dietary fiber, and good hydration. It's cohesive enough to stay intact during evacuation but soft enough to pass without any straining or discomfort.
Types 5, 6 & 7: Hypermotility and Diarrhea
Type 5 appears as soft, distinct blobs with relatively clear edges. Easy to pass, yes — but that morphology suggests transit is moving too fast, or there's not enough dietary bulk (insoluble fiber) to bind the waste together properly. Type 6 is fluffy, poorly defined pieces with ragged, mushy edges. That's significant hypermotility — the colon is expelling waste before it's had a chance to absorb adequate water, and it often comes with a strong sense of urgency. Finally, Type 7 is entirely liquid with no solid matter at all. That's clinical diarrhea, caused by a severe breakdown in the colonic mucosa's ability to absorb water — typically triggered by viral or bacterial infections, acute food poisoning, or a severe inflammatory bowel response.
You can use the tool below to check the Bristol type based on the appearance of your poop.
Bristol Scale Quick Check
Select the image that most closely matches your stool:






Clinical Validation and Epidemiological Data
The Bristol Scale is more than a communication tool — it's a well-validated epidemiological metric backed by real data. In the foundational validation studies by Lewis and Heaton, some striking demographic patterns emerged. The data showed a clear physiological divergence between genders: Types 1 and 2 (constipation) were statistically far more prevalent in women, while Types 5 and 6 (rapid transit) showed up more frequently in men.
The scale also proved instrumental in diagnosing tenesmus — the distressing sensation of incomplete defecation despite an empty rectum. The foundational research found that an overwhelming 80% of individuals reporting tenesmus were actively passing Type 7 stools, which pointed to severe bowel inflammation — not retained fecal matter — as the source of that neurological sense of fullness. Today, routine tracking of Bristol Scale types alongside dietary intake lets both patients and gastroenterologists map these precise physiological correlations, opening the door to targeted interventions in hydration, fiber supplementation, and medical treatment.
Sources & Medical References: