Irritable Bowel Syndrome (IBS): Navigating a Functional Disorder
Understanding the Gut-Brain axis, diagnostic subtypes, and evidence-based lifestyle management.
Beyond "Spastic Colon": What is IBS?
IBS goes by a lot of names — spastic colon, nervous bowel, mucous colitis — but those older labels don't really capture what's happening. It's a functional gastrointestinal disorder, and that word "functional" is worth unpacking: blood tests, biopsies, and colonoscopies all come back looking perfectly normal. No inflammation, no tumors, no structural damage. The problem isn't what your gut looks like — it's how it behaves and communicates with the central nervous system.
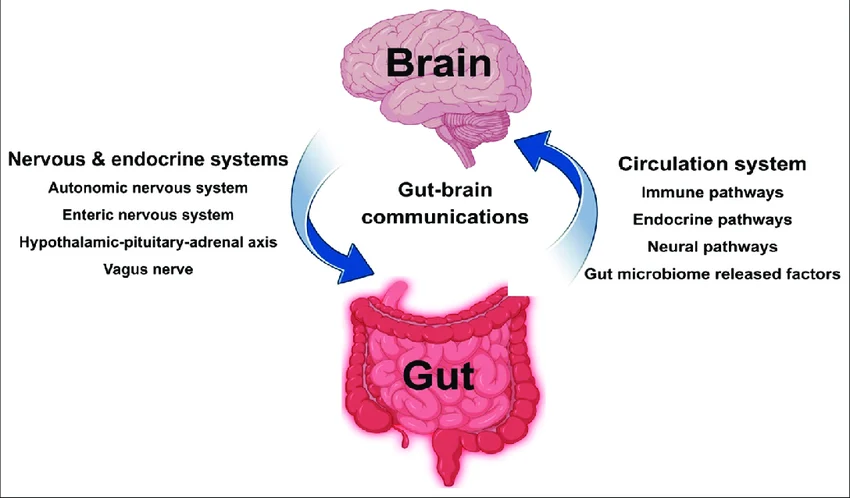
Today's medical consensus views IBS as a disorder of the Gut-Brain Axis. Your enteric nervous system — the dense web of neurons governing your GI tract — runs on hyperdrive. The phenomenon is called visceral hypersensitivity: normal amounts of gas or ordinary digestive contractions that most people never even notice can register in an IBS patient's brain as severe, cramping pain. The signal is real. The gut is just amplifying it far beyond what's warranted.
The Four Clinical Subtypes
IBS doesn't look the same in everyone — it really can't, given how varied the symptoms are. That's why the Rome IV diagnostic criteria divides the disorder into four distinct subtypes, based on your predominant stool pattern, typically assessed using the Bristol Stool Scale.
- IBS-D (Diarrhea-Predominant): The digestive system moves too rapidly. Stools are frequently loose, watery (Bristol Types 6 & 7), and accompanied by a sudden, intense urgency to defecate.
- IBS-C (Constipation-Predominant): The digestive system moves too slowly. Stools are hard, lumpy (Bristol Types 1 & 2), and difficult to pass, often leading to severe bloating and feelings of incomplete evacuation.
- IBS-M (Mixed/Alternating): The patient experiences wild swings in bowel habits, alternating between severe constipation and sudden diarrhea within the same month or even the same week.
- IBS-U (Unclassified): Symptoms of pain and discomfort are present, but bowel habits do not neatly fit into the D, C, or M categories.
Demographics and The Gender Divide
The numbers here are striking: women are two to three times more likely to be diagnosed with IBS than men, and up to five times more likely to seek specialized GI care. Researchers point to a mix of biological and psychosocial factors. On the biological side, hormonal shifts are a major driver — many women with IBS notice a significant worsening of symptoms at specific points in their menstrual cycle.
On the psychosocial side, there's a well-documented link between severe psychological trauma — particularly a history of sexual abuse — and the later development of functional GI disorders. Chronic stress permanently recalibrates the sensitivity of the gut-brain axis, which helps explain why marginalized populations face a disproportionately higher risk.
Red Flag Symptoms: When It Isn't IBS
IBS is a diagnosis of exclusion — meaning doctors need to rule out more serious conditions like Inflammatory Bowel Disease (Crohn's) and colorectal cancer before landing on an IBS diagnosis. Seek immediate medical attention if you experience any of these "red flag" symptoms, because they are not caused by IBS:
- Unintentional and rapid weight loss.
- Nocturnal diarrhea that wakes you from deep sleep.
- Rectal bleeding or stools that appear black and tarry.
- Unexplained iron-deficiency anemia or persistent vomiting.
Management and Relief Strategies
There's no pharmaceutical cure for IBS — but that doesn't mean you're stuck with it. With the right dietary and lifestyle changes, it's genuinely manageable for most people.
- The Low-FODMAP Diet: A medically supervised elimination diet that temporarily restricts Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols—specific carbohydrates that the small intestine struggles to absorb, leading to rapid fermentation and gas production in the colon.
- Data Tracking: Keeping a meticulous daily diary of meal times, specific ingredients, psychological stress levels, and resulting bowel movements is the most effective way to identify personal trigger foods.
- Psychological Interventions: Because of the gut-brain connection, therapies such as gut-directed hypnotherapy, cognitive behavioral therapy (CBT), and even prescribed low-dose antidepressants are frequently used to dull the visceral pain signals traveling from the gut to the brain.
Dietary Management: For many people with IBS, standard dietary advice barely scratches the surface. Clinical protocols like the Low-FODMAP Diet can be genuinely life-changing. The most effective way to figure out which specific foods trigger your symptoms? Use Happy Poop to keep an accurate daily food and symptom diary — it connects the dots so you don't have to guess.
Sources & Medical References: