Understanding Diarrhea: Pathophysiology, Causes, and Clinical Management
A deep dive into the biological mechanisms of bowel hypermotility, malabsorption, and effective rehydration strategies.
The Physiology of Normal Digestion
Let's start with just how efficient your gut normally is — because the numbers are genuinely impressive. Every day, the average human gut processes roughly 9 liters of fluid — that's ingested food and water combined with salivary, gastric, biliary, and pancreatic secretions. The small intestine absorbs the lion's share of this (about 7.5 liters) along with vital nutrients, and the remaining 1.5 liters passes to the large intestine (colon), which absorbs nearly all remaining water and salts. The end result? A healthy person excretes only about 150 to 200 milliliters of fluid in solid feces per day. Diarrhea happens when this finely tuned system breaks down.
The Mechanisms of Diarrhea
Clinically, diarrhea is defined as the passage of three or more loose or liquid stools per day, or more frequently than is normal for you. It's not just a symptom of "eating something bad" — it's a specific biological response that falls into two core pathophysiological categories: osmotic and secretory.
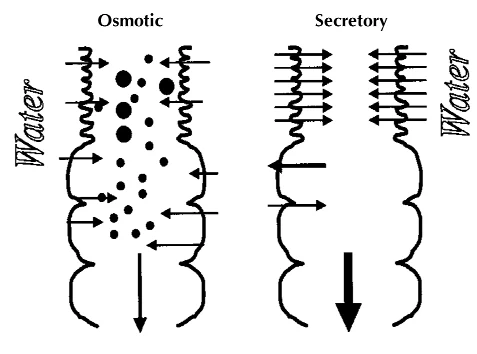
Osmotic diarrhea occurs when unabsorbable, water-soluble solutes stay in the bowel and pull water into the colon rather than letting it be absorbed — you see this clearly in lactose intolerance, where undigested milk sugars act like a sponge in the intestines. Secretory diarrhea is a different beast: here, the intestinal wall actively pumps large volumes of electrolytes and water into the bowel lumen, overwhelming the colon's ability to keep up. Cholera and certain strains of E. coli are the classic examples.
Acute vs. Chronic Diarrhea: Common Causes
Duration matters a lot when it comes to diarrhea. Acute diarrhea comes on suddenly and usually clears up within 5 to 10 days. Chronic diarrhea, on the other hand, persists for more than 4 weeks — and at that point, you need medical investigation to rule out something more serious.
Infectious Gastroenteritis (Acute)
Intestinal infections are the leading cause of acute diarrhea worldwide, and infants and young children are the most vulnerable demographic. Viral pathogens — particularly norovirus and rotavirus — are highly contagious and frequently spark localized outbreaks. Bacterial food poisoning, often caused by Salmonella, Campylobacter, or Escherichia coli, typically comes from contaminated water, undercooked poultry, or unpasteurized dairy.
Pharmacological Triggers and The Gut Microbiome
Medications are frequent culprits of bowel dysregulation. Antibiotics indiscriminately wipe out both pathogenic and beneficial gut bacteria, leading to what's known as antibiotic-associated diarrhea. Certain blood pressure medications, magnesium-containing antacids, and excessive laxative use can also push bowel contents through too quickly for adequate absorption.
Systemic and Functional Disorders (Chronic)
When diarrhea turns chronic, it's usually a signal that something bigger is going on — a systemic or autoimmune condition driving the symptoms. Irritable Bowel Syndrome (IBS) frequently presents with diarrhea (IBS-D), driven by visceral hypersensitivity and hypermotility. Endocrine disorders like hyperthyroidism can rev up the body's metabolic rate and push waste through the digestive tract before adequate absorption occurs. Autoimmune conditions such as Celiac disease or Inflammatory Bowel Disease (Crohn's and Ulcerative Colitis) go further still — they physically destroy the mucosal lining, leaving the gut unable to absorb nutrients or fluids.
Treatment, Prevention, and Management
The real clinical danger of diarrhea isn't the loose stools themselves — it's the dehydration and electrolyte imbalance that follow. Losing significant amounts of water, sodium, potassium, and bicarbonate can trigger severe cardiovascular and neurological complications, and this risk is especially acute in children and elderly adults.
Oral Rehydration Therapy (ORT)
ORT is the cornerstone of diarrhea management, and it's deceptively simple. The treatment involves a precise ratio of water, glucose, and sodium. The glucose isn't there for energy — it activates sodium-glucose co-transporters in the intestinal lining, essentially tricking the gut into absorbing water even while it's actively secreting fluid. That mechanism is why ORT is considered one of the most significant medical advances of the 20th century, dramatically cutting the need for hospitalization across the globe.
Nutritional and Supplemental Interventions
For a long time, patients were told to "starve a fever" and hold off on eating during a severe bout. Modern gastroenterology strongly opposes this. Fasting for more than 4 hours actually makes things worse by degrading the intestinal lining further. Normal feeding should resume as soon as basic rehydration is achieved. The WHO also strongly recommends supplemental zinc therapy for children — it's been shown to reduce the severity of the episode and help prevent future occurrences for up to three months.
Sources & Medical References: