What Causes Constipation? The Physiology of Colonic Transit
Understanding the biomechanics of water absorption, pelvic floor coordination, and delayed bowel motility.
The Biological Mechanism of Constipation
Constipation starts with the colon. As food moves through the stomach and small intestine, vital nutrients are absorbed, leaving a liquid slurry of waste (chyme). When this waste enters the colon, the body begins a careful reclamation process: the colon's primary job is to extract water and essential salts from the waste and solidify it into stool.
Constipation happens when transit time—the speed at which waste moves through your digestive tract—slows down too much. When food moves too sluggishly, the colon gets too much time to absorb water. The result is stool that's severely dehydrated, hard, and physically difficult to pass (typically presenting as Types 1 or 2 on the Bristol Stool Scale).
Clinical Symptoms and Presentation
While occasional irregularity is normal, clinical constipation is generally diagnosed when an individual experiences one or more of the following symptoms persistently:
- Having fewer than three complete bowel movements per week.
- Passing stools that are extremely dry, hard, and lumpy.
- Experiencing physical pain or requiring severe straining to pass a stool.
- Feeling a sense of incomplete evacuation (tenesmus), where the bowel still feels full after a movement.
- Accompanying systemic symptoms such as abdominal cramping, severe bloating, and nausea.
Lifestyle and Dietary Triggers
In the absence of underlying disease, the vast majority of constipation cases are driven by modern lifestyle and dietary habits.
- Lack of Dietary Fiber: Fiber acts as a bulking agent. Soluble fiber absorbs water to keep stool soft, while insoluble fiber acts as a "sweeper" to keep things moving. A diet heavy in processed foods, milk, and cheese, but low in vegetables and whole grains, inevitably slows transit time.
- Dehydration: If the body is systemically dehydrated, the colon will aggressively extract as much water as possible from the stool to preserve vital organ function.
- Sedentary Lifestyle: Physical movement stimulates peristalsis (the wave-like muscle contractions of the intestines). A lack of exercise leads to a "lazy" bowel.
- Ignoring the Urge: Repeatedly resisting the urge to have a bowel movement (often due to public restroom anxiety or busy work schedules) gradually desensitizes the nerves in the rectum, leading to chronic impaction.
The Hydration Connection
Because colonic transit is so heavily reliant on water, increasing fiber without increasing fluid intake can actually make constipation worse. Learn more about how hydration directly impacts your digestion here.
Take Control: The best way to identify what is slowing your transit time is to log your meals, fluid intake, and stool consistency. Start building your personal baseline today by using Happy Poop.
Medical and Pathological Causes
When lifestyle changes don't move the needle, it's time to look deeper. A physician will investigate potential pharmacological or structural causes.
Endocrine and Neurological Disorders
Your digestive system depends on precise hormonal and neurological signaling. Hypothyroidism (an underactive thyroid) slows the entire body's basal metabolic rate, directly dragging down intestinal motility. Neurological conditions like Parkinson's disease, Multiple Sclerosis, and spinal cord injuries disrupt the nerve signals traveling between the brain and the bowel.
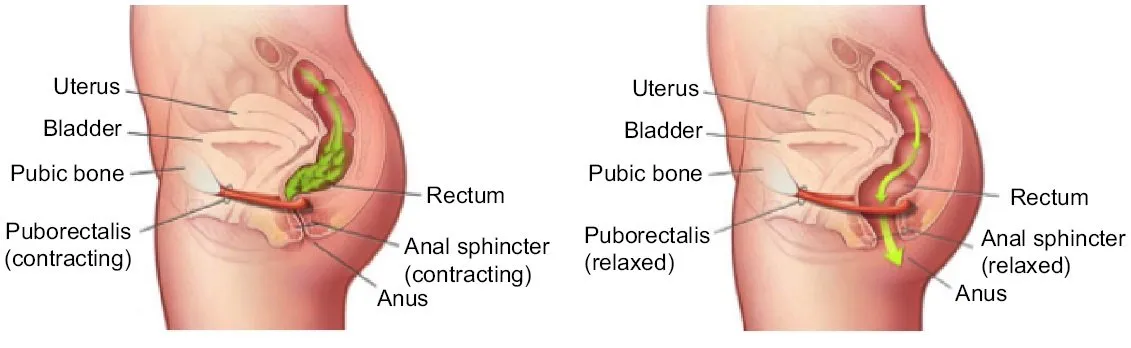
Outlet Dysfunction and Pelvic Floor Issues
Sometimes the colon functions perfectly, but the exit mechanism fails. Outlet Dysfunction Constipation occurs due to a defect in the coordination of the pelvic floor muscles. During a healthy bowel movement, these muscles must relax simultaneously as the abdominal muscles contract. If they involuntarily contract instead (dyssynergic defecation), the stool cannot be expelled.
Structural and Systemic Diseases
Underlying structural problems—including intestinal obstructions, strictures, or tumors (including Colorectal Cancer)—can physically block the passage of stool. Systemic diseases like lupus, scleroderma, and amyloidosis can alter the connective tissue and muscle function of the gastrointestinal tract.
Pregnancy and Hormonal Shifts
Women are statistically more prone to constipation, particularly during pregnancy and the postpartum period. Two factors are mainly responsible. First, rising progesterone levels naturally relax smooth muscle tissue throughout the body, which significantly slows intestinal peristalsis. Second, as the fetus grows, the expanding uterus physically compresses the intestines and colon—a mechanical barrier that further slows the passage of waste.
Sources & Medical References: