Overactive Bladder (OAB): Recognizing Symptoms and Restoring Control
Understanding the involuntary contractions of the detrusor muscle and behavioral pathways to clinical management.
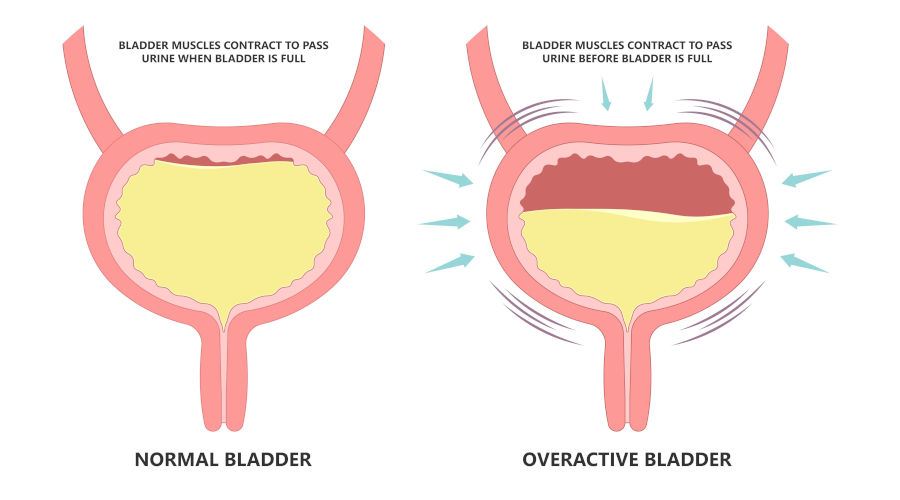
The Mechanics of Urological Control
To get a handle on Overactive Bladder (OAB) syndrome, it helps to start with how the urinary tract is supposed to work. The bladder is a highly elastic, muscular sac that stores urine produced by the kidneys. Its primary wall muscle — the detrusor muscle — stays relaxed as the bladder fills. As it expands, nerve signals travel to the brain indicating that capacity is approaching, giving you plenty of time to find a bathroom. Only when you consciously decide to urinate does the brain give the green light: the urethral sphincters relax, the detrusor muscle contracts, and urine is expelled.
OAB is what happens when that relay breaks down. The detrusor muscle starts contracting on its own — uninvited — triggering a sudden, overwhelming urge to urinate even when the bladder is barely filled.
Clinical Symptomatology
OAB isn't a single disease — it's a cluster of disruptive urinary symptoms affecting millions of adults worldwide. It's more commonly diagnosed in older adults, but here's the thing: it's not a normal or inevitable part of aging, and it should never be dismissed as such.
A diagnosis of OAB is generally considered if a patient regularly experiences the following clinical symptoms:
- Sudden Urgency: The hallmark symptom of OAB. It is characterized by an abrupt, intense, and overwhelming need to urinate that is highly difficult to defer or suppress.
- Urgency Incontinence: This occurs when the sudden urge is so powerful that the detrusor muscle overrides the urethral sphincters, resulting in the involuntary leakage or complete loss of urine before reaching a toilet.
- High Urinary Frequency: The need to urinate eight or more times within a standard 24-hour period, despite normal fluid intake.
- Nocturia: The disruption of the sleep cycle due to the necessity to wake up two or more times per night specifically to urinate. This often leads to chronic fatigue and decreased daytime cognitive performance.
The Psychological and Social Impact
The physical symptoms are disruptive enough — but the psychological toll is just as real. The constant fear of leaking in public pushes many people toward social isolation: limiting travel, reshaping their professional lives, mentally mapping every restroom in every building ("toilet mapping"), and withdrawing from physical intimacy. It's no surprise that OAB is closely linked to elevated rates of clinical anxiety and depression.
First-Line Treatments and Behavioral Management
Since OAB is fundamentally a neuromuscular dysfunction, the first line of treatment isn't medication or surgery — it's behavioral modification and physical therapy. Those come later, if needed.
Bladder Training and Scheduled Voiding
The goal is to gradually stretch the bladder's capacity and retrain the brain to stop responding to those early, false urgency signals. You start by urinating on a strict schedule — say, every hour — whether or not you actually feel the urge. Over time, the intervals are slowly extended, teaching the bladder to comfortably hold larger volumes of fluid.
Pelvic Floor Rehabilitation
Targeted physical therapy — commonly known as Kegel exercises — strengthens the pelvic floor muscles and the external urinary sphincter. When you learn to voluntarily contract those muscles during a sudden urge, you can actually suppress the detrusor contraction before it gets out of control, heading off urgency incontinence before it happens.
Master Your Bladder Training
Retraining an overactive bladder starts with knowing your exact voiding intervals. A strict "voiding diary" lets you safely and gradually stretch the time between bathroom visits. Track your urine frequency, urgency levels, and fluid intake all in one place with Happy Poop.
Sources & Medical References: